(December 2018)

Welcome to the seventh issue of Inside Medicalchain, our monthly newsletter to keep our community up to date.
If you missed the sixth issue you can catch up by clicking here.
Announcement
Medicalchain Opens New Office in Switzerland

Since its foundation, Medicalchain has been growing rapidly and we are delighted to announce the official opening of our new office in Switzerland. We have a global vision and geographical expansion is necessary to achieve this.
Product Development
MyClinic.com continues to improve and we are working to our timeline for version 2 which is eagerly anticipated for the end of Q2 2019.
We are working extra hard to confirm contracts and are hopeful that our services will be available within the NHS as well as the private sector soon.
MyClinic.com will also be available on Android very soon.
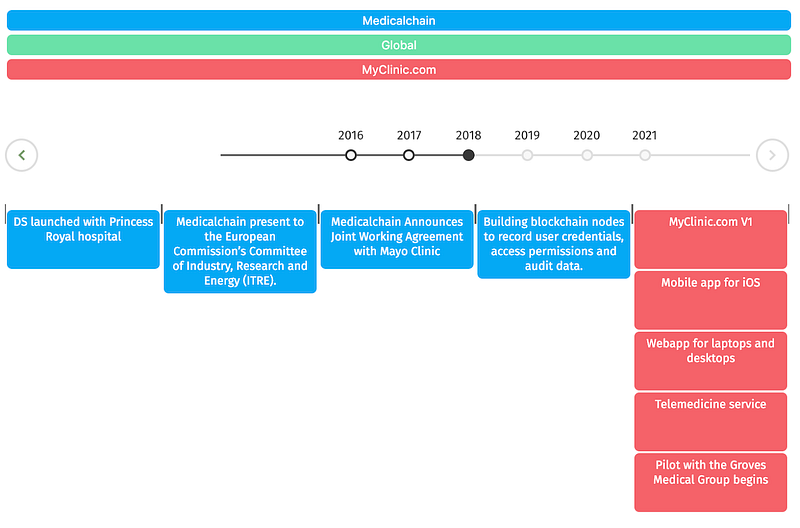
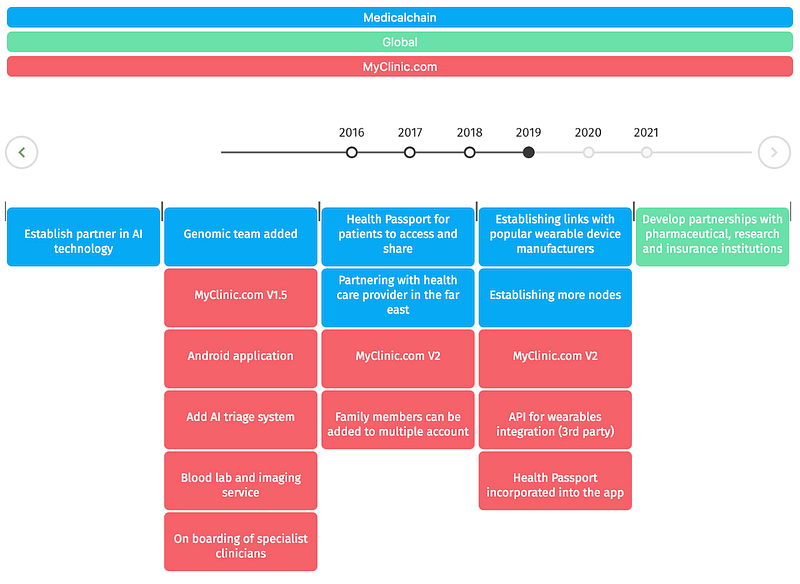
Timeline:
Considering how difficult it can be to keep up with our progress, especially product development — we have created an interactive timeline on our website to update you clearly on our road to achieving our goals.
Want to help? Give us feedback!
Please continue to download our iOS version of the MyClinic.com app and let us know your feedback on version 1.0 by sending us your comments to — [email protected]
Media
Our Communications Manager, Tim Robinson has been working on a new blog about the problems in healthcare and how to address these. Check out some of his articles below:
- Faxploit: Read about the security dangers healthcare systems have by using fax machines — read here
- Lifestyle Intervention: Read about how the NHS plans to help patients at risk of developing diabetes with “lifestyle interventions” to curb the demand the health service is under — read here
- Curiosity killed the…Trust?: Trust is especially valuable when it comes to our intimate health data, read about how that ‘trust’ is being handled today — read here
- E-Prescribing for NHS Trusts: Read about the benefits of “E-Prescribing for NHS Trusts” — read here
- Youth Turning to Apps for Mental Health Needs: Read why our youth are turning to health tech and apps to care for their mental health needs instead of existing conventional options — read here
- Snail Mail in the digital age: Read how using ‘Snail Mail in the digital age’ to inform patients about their vital NHS healthcare services has caused serious delays in tests and screenings for thousands of patients — read here
Events

Our COO, Mo Tayeb has been busy this month in Switzerland, Italy and Taiwan, speaking at various events and forums that showcase the latest in technology in healthcare. In Switzerland, he attended the Life Sciences Leader Forum. In Italy, he spoke at the Futureland event, which highlighted the companies and technologies that are going to make an impact in 2019. Finally, in Taiwan, he presented Medicalchain at the Healthcare Expo at the end of November. This event marks the principal display of solutions and connections for medicine and healthcare in Asia.

Back home, Mo has been just as busy speaking in London at the Healthcare Unblocked event, the UK’s first conference dedicated to advancing blockchain in healthcare.

More in London this month as our Head of Business Development, Dr Amina Albeyatti attended the Giant Health Event 2018 at Stamford Bridge, home to the Chelsea Football Club. We received a warm reception and presented Medicalchain and MyClinic.com and its application in our health, to a very excited audience.

Dr Amina Albeyatti was interviewed by Disruptive Live. Check out the interview below:
https://www.youtube.com/watch?v=hq7-DIRqqRo
We were also interviewed by Jessica DaMassa, health blogger for WTF Health.
As one of the UK’s technology startups and the first UK-based company to bring blockchain technology to healthcare, we were delighted to be invited to the 11th Annual GovNet Parliamentary Awards, hosted by Rt Hon. Baroness Golding. It was an enjoyable and relaxed evening to set off the Christmas season.

Upcoming Events
Our founders will be holding an AMA on December 24th at 7:30 am GMT, a link to the event on YouTube will be shared via our social media closer to the date. Please start posting your questions from now to Communications Manager, Tim Robinson. [email protected]
London January 9th 2018
Designing a Central Bank Digital Currency and Building Healthcare on Blockchain
Medicalchain’s COO, Mo Tayeb, will be speaking at this event. Find out more and how to join us
Social Media
Thank you to everyone who has taken the time to ask us questions and engage with our communications team. If you have not had the chance to say hello yet, please click on one of the links!
Join a Medicalchain Community Today!
- Telegram (English)
- Telegram (Japanese — Medicalchain 日本公式コミュニティ)
- Telegram (Chinese — Medicalchain 官方中文群)
- Telegram (Italian — Medicalchain Italia)
- Telegram (Korean — Medicalchain 공식채팅방)
- Korean Kakao Chat
- Twitter (Japanese)
- Medium
- Youtube
Don’t Forget To Sign Up For Your Free Health Passport
The Medicalchain Health Passport signup is live! Prospective patients and medical practitioners can register their interest now, by clicking here.
Next Issue
- Partnerships within the NHS and private sector
- New website reveal — coming soon
Special thanks
This month marks the end of an eventful year for Medicalchain. With the conceptualisation and delivery of the first rendition of the MyClinic.com application, to the plethora of events all around the world that members of the team have presented at.
We appreciate all the support we have received for what we are trying to achieve, from our loyal community members to representatives we meet at our events — including the wider public at large.
Overall this year we have represented at over 52 events in over 25 cities around the world!
We look forward to the new year and all that we have in line to achieve in keeping with our roadmap. Notably, the updated versions of the MyClinic.com application and the release of the Health Passport, which will truly enable patients to hold their own data. With more good news on the way with exciting partnerships close to being announced.
Again, we thank you for your support and wish you all a Merry Christmas and a Happy New Year, from all at the Medicalchain team.
Thanks for reading the seventh newsletter of Inside Medicalchain. For more information on where to purchase our tokens (MTN), click here.
If you liked it, give it a clap! If you loved it, give us a follow.
Follow the development of Medicalchain on Facebook, Twitter, Instagram, and join the community on Telegram.